The 2026 ACC/AHA Guidelines Changed How Heart Risk Should Be Measured.
We Were Already There.
The most significant update to cardiovascular risk standards in nearly a decade. You will find these reflected in every one of our Cardiometabolic Risk Assessments, as of April 2, 2026.
Updated April 2, 2026
5+
Years
The Cardiometabolic Risk Assessment has included Lipoprotein(a) screening, integration with CAC scores, and ApOB as a clinical tarisk-reduction target since our earliest Assessments delivered in 2001.
40+
Risk Factors
The multiple guidelines from the ACC, NLA, EAS, AHA, ADA, and AACE all endorse a comprehensive approach of considering many clinical risk factors in addition to lab-drawn biomarkers.
100%
Aligned
Each Cardiometabolic Risk Assessment provides you confidence that the report is 100% aligned with the most current published guidelines with nothing missed, left out, or inferred.
35
Years
The Cardiometabolic Risk Assessment is built from the 35+ years of clinical and research experience in lipidology of our Chief Medical Officer, William Cromwell, MD.
0
Alternatives
No other service gives you a complete personalized Assessment that includes the most current ACC/AHA guidelines adjusted for each of your patients to guide an objective clinical discussion..
THE 2026 GUIDELINE ON THE MANAGEMENT OF DYSLIPIDEMIA
The Most Significant Update to Cardiovascular Risk in a Decade
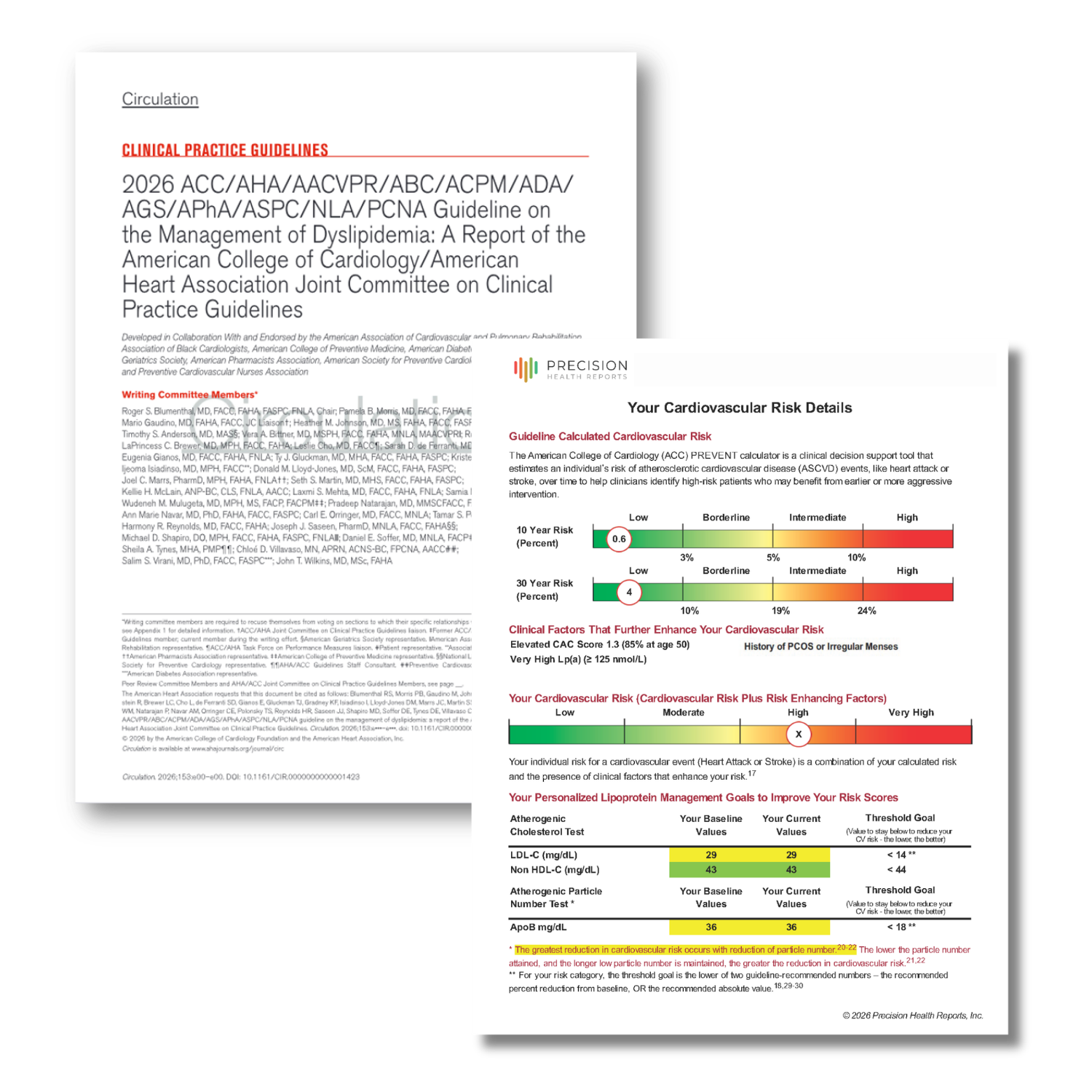
In March 2026, the American College of Cardiology, the American Heart Association, and a consortium of partner specialty societies published the 2026 Guideline on the Management of Dyslipidemia. This is the first comprehensive revision to cardiovascular risk assessment standards since 2018. The authors reviewed more than a decade of accumulated clinical evidence and arrived at changes that reshape how cardiometabolic risk should be calculated, communicated, and acted on.
The most consequential change is the replacement of the Pooled Cohort Equations (PCE) with the AHA PREVENT calculator as the recommended starting point for 10-year cardiovascular risk estimation. PREVENT is better calibrated across a broader, more diverse population. It incorporates kidney function and hemoglobin A1c—two factors with meaningful cardiovascular relevance that the PCE ignored. And it produces risk estimates that are more accurate and less prone to the systematic overestimation that made the PCE increasingly unreliable for many patients. The 2026 guidelines assign PREVENT a Class of Recommendation I designation which is the highest level of endorsement in clinical guideline language.
The guidelines also recalibrate the risk tier thresholds that determine who qualifies for which level of intervention. Because PREVENT produces lower scores than PCE for the same patient, the "high risk" threshold was moved from ≥20% to ≥10% on the 10-year ASCVD risk scale. This means a substantial population that would have been classified as intermediate risk under the old model now qualifies for aggressive LDL-lowering therapy, including high-intensity statin therapy and LDL-C targets below 70 mg/dL. That reclassification is one of the most clinically significant changes in the entire document.
Beyond the calculator, the guidelines elevate several biomarkers and clinical factors from optional to required or strongly recommended. Universal Lp(a) measurement, a genetically inherited risk factor present in roughly one in five adults, is now a Class I recommendation for all adults, with cascade screening of first-degree relatives when Lp(a) is elevated. Apolipoprotein B (ApoB) is formally endorsed as a co-primary treatment target alongside LDL-C. Coronary artery calcium scoring retains its Class I status as a decision aid for borderline and intermediate-risk patients. And the set of recognized women's reproductive health risk-enhancing factors is meaningfully expanded.
“The shift from PCE to PREVENT isn’t a minor recalibration. It changes who gets flagged for treatment and when. More importantly, it changes the treatment targets that follow.”
SOURCE CITATION
Blumenthal RS, et al. 2026 ACC/AHA/Multisociety Guideline on the Management of Dyslipidemia. Journal of the American College of Cardiology. 2026; Article in Press.
HOW THE THRESHOLDS CHANGED
The Definition of High Risk Just Changed
When the risk calculator changes, the thresholds that define each risk tier have to change with it. Here is what that looks like and why it matters clinically.
QUICK REFERENCE
How PREVENT Changed the Risk Thresholds
The Cardiometabolic Risk Assessment from Precision Health Reports is aligned with the lastest PREVENT risk tiers. These are starting points before also considering Risk Enhancing Factors.
| Risk Tier | Prior Standard Pooled Cohort Equation | 2026 Standard AHA PREVENT Calculator ✓ PHR Aligned |
|---|---|---|
| Low | < 5% | < 3% |
| Borderline | 5 – 7.5% | 3 – <5% |
| Intermediate | 7.5 – <20% | 5 – <10% |
| High | ≥ 20% |
≥ 10%
Threshold cut in half |
The high-risk threshold was cut in half. Patients with a 10-year PREVENT risk between 10–19% now qualify for LDL-C targets below 70 mg/dL and high-intensity statin therapy.
Source: Blumenthal RS, et al. 2026 ACC/AHA Dyslipidemia Guideline.
While we implemented PREVENT into all Cardiometabolic Risk Assessments in December 2025, we were using the previously higher thresholds for each risk tier. With this new guideline release, we have updated the risk tiers that you will see in the Cardiovascular Risk Details portion of every report.
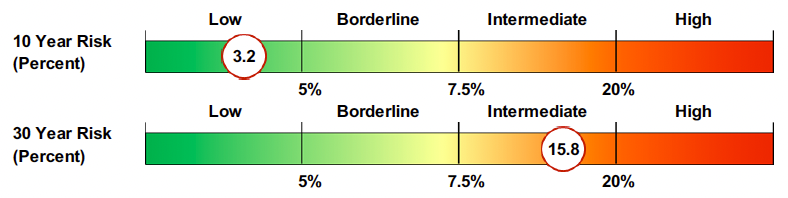
Previous Risk Tier Example
New Risk Tier Example
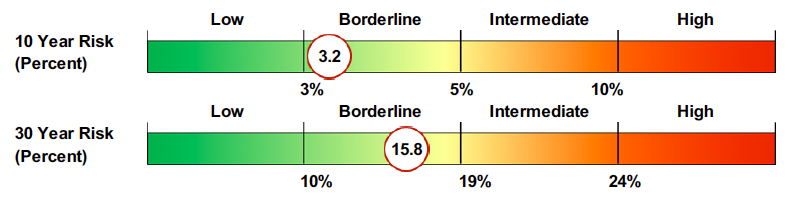
The high-risk threshold was cut in half. Patients with a 10-year PREVENT risk between 10–19% (previously classified intermediate) now qualify for LDL-C targets below 70 mg/dL and an honest discussion about starting statin therapy. Similarly, the 30-year risk tiers shifted slightly as well.
The Cardiometabolic Risk Assessments reflect these updated thresholds as of April 2, 2026.
FULL GUIDELINE ALIGNMENT
Where Precision Health Reports Stands on Every Major Change
Precision Health Reports is built on a guideline-based clinical methodology which means we can align to new standards the moment they're published. Here is how each major element of the 2026 update maps to what the Cardiometabolic Risk Assessment already does.
| Guideline Element | 2026 ACC/AHA Requirement | PHR Status | PHR Adoption |
|---|---|---|---|
| PREVENT Calculator | Class I recommendation — replaces the Pooled Cohort Equation (PCE) as the standard 10-year ASCVD risk estimator. | Aligned | Dec 2025 3 months before mandate |
| Updated Risk Tier Thresholds | New PREVENT-based cutoffs: Low <3%, Borderline 3–<5%, Intermediate 5–<10%, High ≥10%. | Aligned | Apr 2026 |
| Lp(a) Measurement | Class I recommendation — universal screening for all adults; cascade testing of first-degree relatives when Lp(a) is elevated. | Aligned Includes cascade guidance | Since 2021 Since launch |
| ApoB as Co-Primary Target | ApoB formally endorsed alongside LDL-C for risk assessment and treatment monitoring across all risk tiers. | Aligned | Since 2022 |
| CAC Scoring | Class I recommendation for risk stratification in borderline and intermediate-risk patients. | Aligned Integrated into PHR risk stratification | Since 2021 Since launch |
| Women's Reproductive Risk Markers | Expanded set of reproductive and women's health conditions recognized as cardiovascular risk-enhancing factors. | Aligned Questionnaire updated Apr 2026 | Apr 2026 |
All Precision Health Reports Cardiometabolic Risk Assessments also incorporate systemic inflammation, insulin resistance, South Asian ethnicity, metabolic syndrome, CKD (stages 3–4), chronic inflammatory conditions (RA, SLE, psoriasis, HIV), and 20+ additional guideline-endorsed risk-enhancing factors not shown above.
2026 GUIDELINE UPDATE
More Complete. More Personalized for Women’s Health.
The 2026 guidelines formally expand the set of reproductive and women's health conditions recognized as cardiovascular risk-enhancing factors. Conditions including hypertensive disorders of pregnancy, gestational diabetes, and premature menopause now carry explicit guideline endorsement, meaning they should prompt earlier and more serious consideration of lipid-lowering therapy when present alongside borderline or intermediate risk scores.
The Cardiometabolic Risk Assessment Preassessment Questionnaire has been updated to capture all of these conditions. They are incorporated automatically into every assessment's risk-enhancing factor analysis. For health systems and DPC practices running programs that serve women, including occupational health programs, this update ensures no clinically recognized risk factor goes uncaptured.
Cardiovascular Risk Enhancing Factors Specifically for Women
Preeclampsia or Eclampsia
Early Onset Menopause
History of Gestational Diabetes
History of Gestational Hypertension
History of Preterm Delivery
History of Small for Gestational Age Birthweight
History of Recurrent Spontaneous Pregnancy Loss
History of Early Menarche
History of Polycystic ovarian syndrome (PCOS)

FROM OUR CHIEF MEDICAL OFFICER
Built by Someone Who's Been in Your Clinical Shoes for 35 Years

“Cardiovascular guidelines don't change casually. When the ACC and AHA move the threshold for high risk from 20% to 10%, that's a meaningful clinical decision with real consequences for real patients. When building Precision Health Reports, we always kept guidelines as our North Star. Every assessment is designed to reflect those decisions the moment they're made to support your clinical discussion with your patients, not months later when everyone else catches up.”
William Cromwell, MD, Chief Medical Officer, Precision Health Reports
Board-Certified Lipidologist. 35+ Years Clinical Practice, Research, and Teaching. 23+ Peer-Reviewed Publications.
FOR CLINICIANS AND HEALTH SYSTEMS
Add Guideline-Aligned Assessment to Your Practice
Less than 30 seconds to order. Patient-facing and clinician-facing reports included. Works with your existing lab.
FOR INDIVIDUALS
Understand Your Heart Risk Under the 2026 Standards
One assessment. Personalized to your biomarkers, history, and risk factors. FSA/HSA eligible.
Sources and Related Reading
Background: From Framingham to PREVENT—The Evolution of Cardiometabolic Risk Assessment
For individuals: What the 2026 Guidelines Mean for Your Assessment
This page reflects Precision Health Reports’s clinical assessment methodology as of April 2, 2026. Guideline source: Blumenthal RS, et al. 2026 ACC/AHA/Multisociety Guideline on the Management of Dyslipidemia, JACC 2026. PHR's methodology is reviewed and updated by Chief Medical Officer Dr. William Cromwell in response to major guideline publications.