hsCRP (High-Sensitivity C-Reactive Protein): Inflammation and Cardiometabolic Risk
Learn how hsCRP (high-sensitivity C-reactive protein) measures systemic inflammation and predicts cardiovascular risk. Understand interpretation, optimal ranges, limitations, and how hsCRP compares to GlycA in Precision Health Reports Assessments.
What Is hsCRP?
High-sensitivity C-reactive protein (hsCRP) is a laboratory test that measures very low levels of C-reactive protein in the blood, a protein produced by the liver in response to inflammation.
Unlike standard CRP tests, which detect large inflammatory responses such as infection or trauma, hsCRP is designed to quantify low-grade systemic inflammation. This type of chronic inflammation plays a central role in:
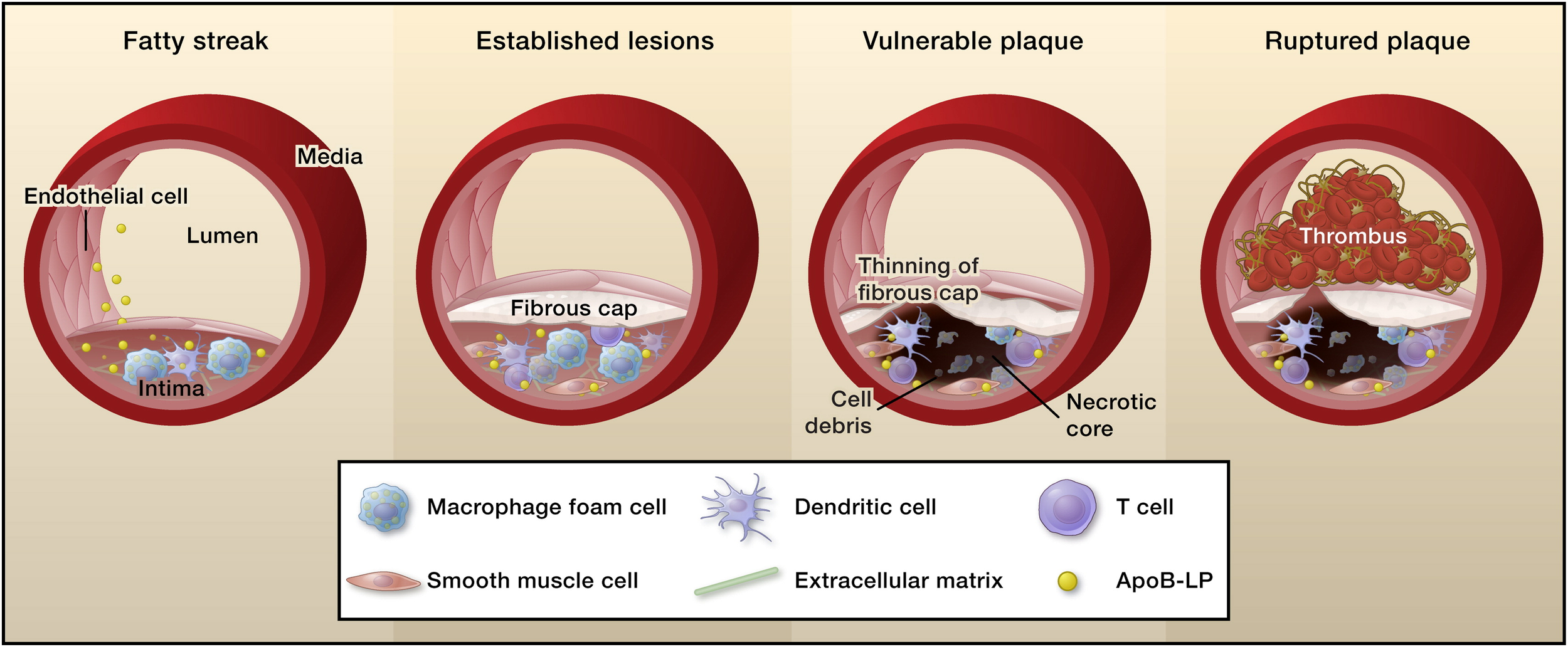
Atherosclerosis
Plaque instability
Insulin resistance
Cardiometabolic disease progression
hsCRP is one of the most extensively studied inflammatory biomarkers in cardiovascular medicine and is incorporated into major risk assessment frameworks, including guidance from the American College of Cardiology and the American Heart Association.
Why Inflammation Matters in Cardiometabolic Disease
Cardiometabolic disease is not simply a cholesterol storage disorder. It is a dynamic inflammatory process involving:
Endothelial dysfunction
Lipoprotein retention in the arterial wall
Immune activation
Progressive plaque formation
Inflammation amplifies every step of this cascade. Elevated hsCRP has been shown to predict:
Myocardial infarction
Ischemic stroke
Peripheral arterial disease
Cardiovascular mortality
Importantly, hsCRP provides risk information independent of LDL cholesterol and ApoB levels.
hsCRP and Cardiovascular Risk Prediction
Evidence From Landmark Clinical Trials
Several major trials established hsCRP as a clinically meaningful risk marker:
Demonstrated that individuals with normal LDL but elevated hsCRP benefited from statin therapy, with significant reductions in cardiovascular events.
Showed that targeting inflammation directly reduced cardiovascular events, independent of lipid lowering.
These studies reinforced a critical concept: Cardiovascular risk is driven by both lipid burden and inflammatory activity. hsCRP serves as a practical clinical window into that inflammatory component.
Interpreting hsCRP Levels
| hsCRP (mg/L) | Typical Interpretation |
|---|---|
| < 1.0 | Lower inflammatory risk profile; commonly seen in metabolically healthy individuals. |
| 1.0–2.9 | Average background inflammation; interpret in context of other risk markers (ApoB, blood pressure, glycemic status). |
| 3.0–9.9 | Higher chronic inflammation signal; associated with elevated cardiovascular risk in many cohorts. Consider repeat testing if recent illness is possible. |
| ≥ 10.0 | Often reflects acute inflammation (infection, injury, flare). Defer cardiovascular risk interpretation and repeat when clinically stable. |
hsCRP is non-specific and can rise with infection, trauma, autoimmune disease, recent surgery, vigorous exercise, or smoking. Many guidelines recommend repeating hsCRP (often 2 measurements, ideally ~2 weeks apart) when the initial value is elevated, and avoiding interpretation if hsCRP is ≥10 mg/L until rechecked when you are well. For cardiometabolic prevention, hsCRP is best interpreted alongside lipid burden (ApoB or LDL-P), metabolic health (A1c, fasting glucose/insulin), blood pressure, body composition, family history, and overall clinical context in consultation with a qualified clinician.
Important Interpretation Considerations
hsCRP should not be measured during acute infection or illness.
Levels above 10 mg/L usually reflect transient inflammation.
Serial measurements may improve reliability.
Results must be interpreted alongside lipid markers (ApoB), metabolic markers (HOMA-IR), and clinical context.
In isolation, hsCRP does not diagnose disease. It refines risk.
hsCRP vs. GlycA: How They Compare
| Feature | hsCRP | GlycA |
|---|---|---|
| What it measures | C-reactive protein concentration (acute-phase reactant), using a high-sensitivity assay. | Composite NMR signal from glycosylated acute-phase proteins (a broader inflammatory signature). |
| Primary clinical use | Risk refinement for cardiometabolic prevention and cardiovascular events; widely used in practice. | Risk refinement and inflammation tracking; increasingly used where NMR-based testing is available. |
| Guideline footprint | Referenced in major prevention guidance as a risk-enhancing factor in appropriate contexts. | Growing evidence base; less commonly included as a named marker across broad guidelines. |
| Availability | WIDELY AVAILABLE Commonly offered by most clinical laboratories. | LIMITED AVAILABILITY Typically requires NMR-based platforms and may be lab-network dependent. |
| Stability over time | MORE VARIABLE Can rise with infection, injury, autoimmune flare, vigorous exercise, or recent illness. | MORE STABLE Often less sensitive to short-term fluctuations compared with hsCRP. |
| What can confound results | Acute illness is a major confounder; values ≥10 mg/L often suggest deferring interpretation and retesting when well. | Still influenced by inflammatory states, but typically shows fewer sharp “spikes” from transient illness. |
| Best use case | Practical, validated inflammation measurement when you need a broadly accessible marker. | A strong option when NMR-based testing is available and you want a stable inflammatory signal over time. |
| How Precision Health Reports uses it | Used as the primary inflammation marker in the rebuilt assessment when GlycA is not available. | Used in flagship offerings where LabCorp analytes are available, as a high-quality inflammation signal. |
Practical note: Because hsCRP can rise transiently, repeat testing (often two measurements, ideally separated by about two weeks) may help confirm a stable baseline when the initial hsCRP is elevated. GlycA and hsCRP are best interpreted alongside lipid burden (ApoB or LDL-P), insulin resistance markers (HOMA-IR), glycemic markers (A1c), blood pressure, and clinical context.
At Precision Health Reports:
When advanced NMR-based markers such as GlycA are available, they provide a highly stable inflammation signal.
When GlycA is not available, hsCRP serves as a robust, guideline-supported, and clinically validated near-peer alternative for inflammation assessment.
The goal is not to elevate one biomarker above the other universally. The goal is to use the best available data within each clinical setting.
When Is hsCRP Most Clinically Useful?
Inflamatory biomarkers like hsCRP add the most value when:
Lipid levels indicate an ASCVD risk at borderline or intermediate risk
Traditional risk calculators underestimate risk
There is a family history of premature ASCVD
Metabolic syndrome features are present
A clinician is considering intensifying lipid-lowering therapy
It is particularly useful in individuals with:
Elevated ApoB
Elevated HOMA-IR
Elevated Lipoprotein(a)
In these contexts, hsCRP (or GlycA) helps identify individuals with heightened inflammatory vulnerability.
Limitations of hsCRP
While powerful, hsCRP has limitations:
It is non-specific and rises with infection, trauma, and autoimmune disease.
It may fluctuate more than composite inflammatory markers.
It does not localize inflammation to vascular tissue.
It should not replace lipid burden assessment.
hsCRP should be viewed as one pillar in a multi-marker cardiometabolic strategy.
How hsCRP Fits Into Precision Health Reports Assessments
Precision Health Reports integrates hsCRP into the Cardiometabolic Risk Assessment when GlycA is not available or hsCRP is preferred by the ordering physician. We do this by:
Interpreting inflammation relative to lipid burden (ApoB)
Evaluating inflammatory-lipid discordance
Contextualizing hsCRP within age, sex, ethnicity, and clinical history
Harmonizing results with ACC, AHA, and NLA guidance
Inflammation does not act alone. It interacts with:
Lipoprotein particle burden
Insulin resistance
Glycemic control
Blood pressure
Our approach evaluates hsCRP within that full ecosystem.
FAQs about hsCRP
-
No. hsCRP is a high-sensitivity assay designed to detect low levels of chronic inflammation relevant to cardiovascular disease, whereas standard CRP detects larger inflammatory responses.
-
Yes. If elevated, repeat testing after several weeks can confirm whether the elevation reflects chronic inflammation or temporary illness.
-
Yes. Weight loss, smoking cessation, dietary changes, improved sleep, and regular exercise can reduce systemic inflammation and lower hsCRP levels.
-
No. Cardiovascular risk depends on lipid burden, metabolic status, genetics, and inflammation. A normal hsCRP does not eliminate risk.
-
They measure different aspects of inflammation. When available, GlycA provides a highly stable inflammatory signal. When GlycA is unavailable, hsCRP is a validated, widely accessible, and guideline-supported alternative.
Key Takeaways about hsCRP
hsCRP measures low-grade systemic inflammation.
Elevated hsCRP independently predicts cardiovascular events.
It complements lipid and metabolic biomarkers.
It is widely available and incorporated into major guidelines.
When used at Precision Health Reports Assessments, hsCRP functions as a powerful inflammation marker, especially when advanced NMR markers are not available.
References and Clinical Sources
Landmark Clinical Trials
Ridker PM et al.
Ridker PM et al.
Ridker PM.
Guideline and Scientific Statements
American College of Cardiology / American Heart Association.
2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease.
American Heart Association Scientific Statement.
Markers of Inflammation and Cardiovascular Disease. Circulation.
National Lipid Association.
Recommendations for Patient-Centered Management of Dyslipidemia.
Inflammation and Residual Risk Literature
Libby P.
Inflammation in Atherosclerosis. Nature. 2002.
Ridker PM.
Residual Inflammatory Risk: Addressing the Inflammatory Component of Cardiovascular Disease. European Heart Journal.
Pearson TA et al.
Markers of Inflammation and Cardiovascular Disease: Application to Clinical and Public Health Practice. Circulation. 2003.
hsCRP Risk Stratification Data
Emerging Risk Factors Collaboration.
C-Reactive Protein and Risk of Coronary Heart Disease, Stroke, and Mortality. Lancet link.
Ridker PM et al.
Comparison of C-Reactive Protein and LDL Cholesterol Levels in the Prediction of First Cardiovascular Events. New England Journal of Medicine.