UPDATED APRIL 2026
Your next assessment is the most accurate one yet.
The 2026 ACC/AHA Guidelines changed how cardiovascular risk is calculated, who qualifies for a recommendation for treatment, and what markers matter most. Precision Health Reports reflects every update, so your results reflect the best available science.
WHAT THIS MEANS FOR YOU
The Rules of Cardiovascular Risk Just Changed. Here’s What that Means for Your Numbers.
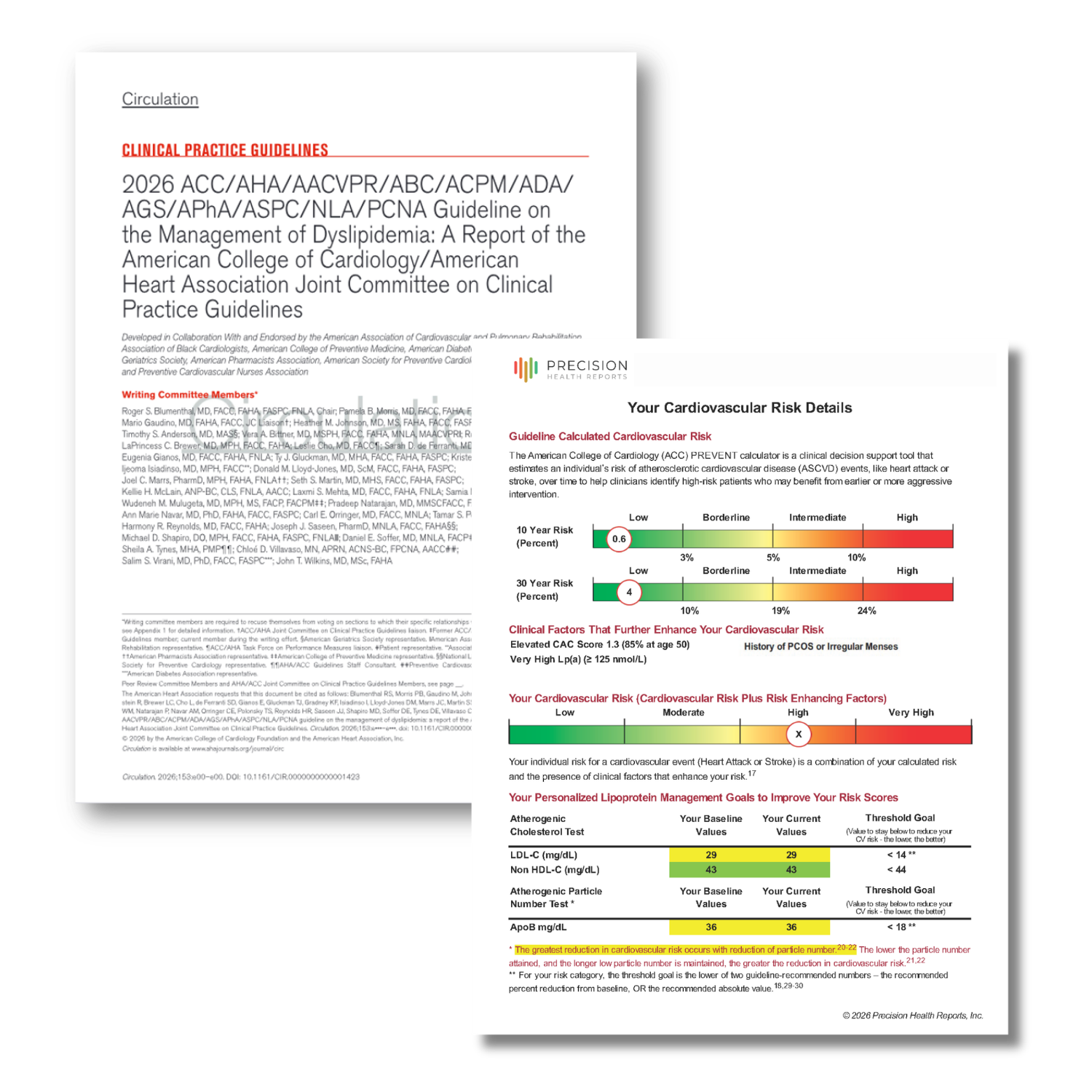
For more than a decade, your cardiovascular risk was calculated using the Pooled Cohort Equation (PCE). The PCE was a model built on older data that didn’t account for kidney function, metabolic health, or how these conditions interact over time. The 2026 ACC/AHA Guidelines officially retire the PCE and replace it with the AHA PREVENT Calculator, which incorporates those factors and produces a more accurate picture of your 10-year risk. Since late 2025, Precision Health Report has used PREVENT by default as the starting point for the Cardiovascular Risk Details portion of every Cardiometabolic Risk Assessment report.
The definition of “high risk” also changed in a way that could directly affect you. Under the old model, you needed a 10-year ASCVD risk of 20% or higher to be classified as high risk. Under the 2026 guidelines, that threshold drops to 10%. That means millions of people who were previously classified as intermediate risk, and may not have been considered for aggressive treatment, now fall into a category where LDL-C targets below 70 mg/dL and high-intensity lipid lowering therapy are recommended by these guidlelines.
Two markers that Precision Health Reports has measured since our launch are now Class I recommendations in the 2026 guidelines, meaning cardiologists are directed to test every adult for them. Lipoprotein(a), or Lp(a), is a genetically inherited marker of cardiovascular risk that standard cholesterol panels miss entirely. ApoB, a direct measure of the number of atherogenic particles in your blood, is now endorsed as a co-primary treatment target alongside LDL-C. If you’ve had a Cardiometabolic Risk Assessment in the past, you already have these numbers. If you haven’t, now is the right time.
Guidelines don’t change often. When they do, it’s because the science has reached a level of consensus that the cardiology community can no longer ignore. The 2026 update is the most significant revision to cardiovascular risk assessment in over a decade. Your assessment should reflect it. Ours does.
Were you told you were “intermediate risk”? That may have changed.
Under the old PCE model, a 10-year ASCVD risk score between 10–19% placed you in the “intermediate risk” category—a designation that often resulted in a “wait and see” approach to treatment.
Under the 2026 ACC/AHA Guidelines, a score of 10% or higher now classifies you as high risk. The guidelines recommend LDL-C below 70 mg/dL and high-intensity lipid-lowering therapy for this group. This is a conversion you and your healthcare provider should have.
If your last assessment was more than a year ago — or if it was done using the old PCE calculator — your risk classification may no longer be accurate.
Get a 2026-Aligned Assessment→
AHEAD OF THE CURVE
We Built this Before it was Required. For You.
Precision Health Reports was founded on the belief that the standard annual physical misses the cardiometabolic risk markers that matter most. Why? Because most physicals use basic labwork and do not personalize the labs values again your risk factors. Long before the 2026 guidelines formalized these recommendations, we built them into every Assessment that we have delivered. The timeline below isn’t a list of compliance dates. It’s a record of what we believed in before we were told to.
The 2026 ACC/AHA Guidelines didn’t change how we work. They confirmed it. Every marker now mandated by the guidelines has been part of your Precision Health Report since we launched.
FOR WOMEN
Women’s Cardiovascular Risk has Never Been Fully Told by Cholesterol Alone.
Women experience cardiovascular disease differently than men, and for decades clinical research underrepresented that difference. The 2026 ACC/AHA Guidelines formally recognize a set of reproductive and hormonal health conditions as cardiovascular risk-enhancing factors that affect a woman’s heart risk independent of her cholesterol levels.
Each of these conditions is now documented in the guidelines as a reason to pursue more aggressive risk management, even when a woman’s standard lipid panel looks normal. Precision Health Reports updated the questions in the Preassessment Questionnaire for women in April 2026 to capture all of these factors. If you are a woman and your previous assessment didn’t ask about your reproductive history, your risk profile may be incomplete.
Cardiovascular Risk Enhancing Factors Specifically for Women
Preeclampsia or Eclampsia
Early Onset Menopause
History of Gestational Diabetes
History of Gestational Hypertension
History of Preterm Delivery
History of Small for Gestational Age Birthweight
History of Recurrent Spontaneous Pregnancy Loss
History of Early Menarche
History of Polycystic ovarian syndrome (PCOS)

The guidelines that are the backbone of our Cardiometabolic Risk Assessment do not change often. As such, these new 2026 guidelines aren’t a small update. They represent a fundamental shift in how we define and manage cardiovascular risk for you and your healthy future. The tools we’ve incorporated into each Cardiometabolic Risk Assessment—PREVENT, Lp(a), ApoB, CAC—are no longer ahead of the curve. They are the curve.
William Cromwell, MD, Chief Medical Officer, Precision Health Reports
Board-Certified Lipidologist. 35+ Years Clinical Practice, Research, and Teaching. 23+ Peer-Reviewed Publications.

Your Risk is Worth Knowing Correctly.
Get a 2026-aligned Precision Health Report and find out exactly where you stand.

A comprehensive and actionable risk assessment report to identify your individual risks for cardiovascular disease, heart attack or stroke, as well as metabolic syndrome and type 2 diabetes.
Note: Available to residents 18 years of age and older in the U.S. only (for now).
You should only order our risk assessment products if you live within a reasonable distance to a LabCorp Patient Service Center (PSC). We will send you an order for a single LabCorp visit to have your blood drawn. Find your nearest LabCorp facility.
Sources
Blumenthal RS, et al. 2026 ACC/AHA/Multisociety Guideline on the Management of Dyslipidemia. Journal of the American College of Cardiology. 2026; Article in Press.
Khan SS, et al. 2023 AHA/ACC Guideline for Cardiovascular Risk Assessment using the PREVENT Equations. Circulation. 2024;149:e279–e311.
Lloyd-Jones DM, et al. Use of Risk Assessment Tools to Guide Decision-Making in Primary Prevention. J Am Coll Cardiol. 2019;73(24):3153–3167.
Honigberg MC, et al. Association of Premature Cardiovascular Disease with Reproductive Disorders in Women. JAMA. 2019;322(23):2303–2314.